
In the Bethesda System (TBS) for cervical liquid-based cytology, High-Grade Squamous Intraepithelial Lesion (HSIL) represents a critical diagnostic threshold. It indicates that a cervical lesion has progressed to a stage requiring high clinical vigilance and proactive intervention. Accurate interpretation directly impacts the timeliness and precision of subsequent clinical decision-making. Today, we will systematically review the diagnostic essentials of HSIL.
1. Cell Size:
HSIL cells are generally smaller than LSIL cells and exhibit lower cytoplasmic maturity.
While cell size may vary, HSIL cells are overall smaller than those of LSIL. High-grade lesions often contain a significant population of small, parabasal-type cells.
2. Nucleus:
Nuclear Enlargement: Inconsistent compared to LSIL. Some HSIL cells show nuclear enlargement similar to LSIL but with significantly increased Nuclear-to-Cytoplasmic (N/C) ratios due to decreased cytoplasm. Others have very high N/C ratios but smaller absolute nuclear size (sometimes as small as a normal intermediate cell nucleus).
N/C Ratio: Consistently higher in HSIL than in LSIL.
Hyperchromasia: Nuclei are typically hyperchromatic but can be normochromatic or even pale.
Chromatin: May be fine or coarsely granular, but is uniformly distributed.
Nuclear Membrane: Distinctly irregular contours, often with prominent indentations or notches.
Nucleoli: Generally absent, though occasionally observed, particularly when HSIL involves endocervical gland spaces or occurs in a background of reactive/reparative changes.
3. Cytoplasm:
Displays varied morphology; may appear "immature," delicate/lace-like, or present as dense metaplastic staining. Occasionally, cytoplasm may appear "mature" with dense keratinization (Keratinizing HSIL).
4. Cellular Arrangement:
Cells may occur singly, but typically present in "crowded sheets" or "syncytial-like" aggregates with indistinct cell borders.
Mnemonic: Large hyperchromatic nuclei, high N/C ratio, pleomorphic shapes, and disordered arrangement.
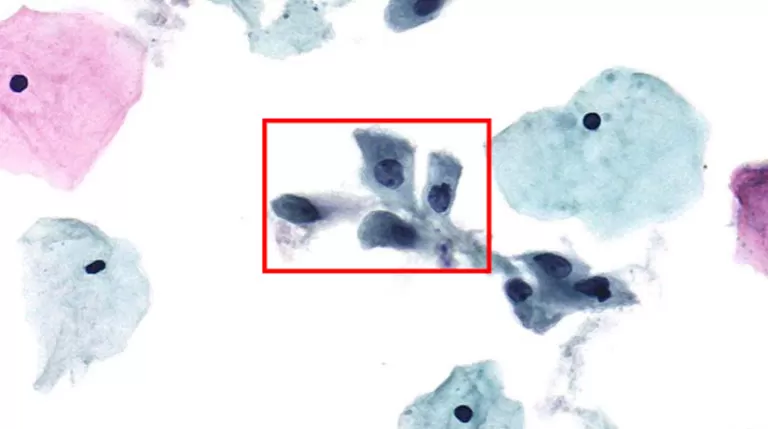
Figure 1: Typical HSIL Morphology Note: Prepared via HealthSky SCTE-3600A SCT Method; Reviewed with HealthSky Patho. AI-Assisted Diagnostic System.
1. HSIL in Atrophic Background:
Challenge: Atrophic epithelial cells are often small with nuclear crowding and high N/C ratios, which may lead to overdiagnosis.
Key Differentiation: HSIL cells exhibit more pronounced nuclear abnormalities (coarser chromatin, more irregular membranes) and create a "discordant" appearance against the atrophic background. Follow-up after estrogen therapy can aid differentiation.
2. HSIL Involving Endocervical Glands:
Challenge: Easily misidentified as glandular lesions or Adenocarcinoma In Situ (AIS).
Key Differentiation: HSIL clusters typically have smooth borders with a "whorled" center, retaining squamous characteristics and disordered nuclear polarity. In contrast, AIS clusters are more organized, exhibiting "feathering," "rosettes," and pseudostratified palisading columnar cells.
3. HSIL with Inflammatory or Reparative Changes:
Challenge: Severe inflammation or repair can cause cellular/nuclear enlargement and prominent nucleoli, mimicking neoplasia.
Key Differentiation: Reparative cells usually have smooth nuclear membranes, fine granular chromatin, and maintained polarity. Irregular nuclear membranes and coarse/clumpy chromatin are hallmarks of HSIL. While nucleoli are rare in typical HSIL, their presence should raise suspicion of potential invasion.
Features | High-Grade Squamous Intraepithelial Lesion (HSIL) | Squamous Cell Carcinoma (SCC) |
Cell Morphology | Relatively consistent; despite atypia, an "epithelioid" structure is maintained. | Marked pleomorphism; bizarre-shaped cells (e.g., spindle cells, tadpole cells) may be present. |
Nuclear Features | Nuclei are large and hyperchromatic, but size remains within a certain predictable range. | Extreme nuclear atypia: extreme variation in size, bizarre shapes, and chromatin appearing as coal-clumps or "ink-drops." |
Nucleoli | Typically inconspicuous or absent. | Large, prominent, multiple, and irregular nucleoli are critical warning signs. |
Background | Usually clean, or may be accompanied by inflammation. | Typical tumor diathesis: necrotic debris (dirty necrotic background), old hemorrhage, and inflammatory cell infiltration. |
Cellular Arrangement | Crowded sheets or syncytial-like aggregates. | Predominantly isolated and scattered distribution, indicating a loss of intercellular cohesion. |
Core Reminder: If you observe prominent nucleoli, extreme pleomorphism, or a diathesis (tumor necrosis) in an HSIL field, the possibility of Squamous Cell Carcinoma (SCC) must be considered immediately and noted in the report.
Clinical management for women with HSIL includes: Colposcopy with cervical biopsy and Endocervical Curettage (ECC) to detect high-grade lesions. Subsequent treatment depends on biopsy results.
Patients ≥ 25 years: If HSIL is cytologically confirmed and a lesion is identified during colposcopy, immediate excision is recommended.
Biopsy-unconfirmed HSIL: If colposcopy fails to identify a lesion after an HSIL cytology result, a thorough review of cytological and histological specimens is required. Additional sectioning and p16 IHC staining may be utilized to reveal occult lesions.
Special Populations (Pregnancy): Colposcopy by an experienced clinician is recommended; however, ECC is unacceptable. If no histological HSIL is found, a follow-up is recommended six weeks postpartum.
Accurate HSIL interpretation is a pivotal link in cervical cancer screening. It requires pathologists to maintain a "keen eye" to capture essential features amidst complex morphologies, distinguish mimics, and remain alert for invasion.
HealthSky is committed to providing premium LBC liquid-based cytology products and services, partnering with you to safeguard women’s cervical health.
 EN
EN
 jp
jp  ko
ko  fr
fr  de
de  pt
pt  ar
ar  es
es  ru
ru  fa
fa  id
id 




